As readers of this blog will know, I have been working in the area of longevity science for over ten years, including helping found the Longevity Center at Sheba Hospital/University of Tel Aviv. My primary interest has been and is still the relationship of sleep to health. I hope to have a lot more to say about that in the coming months.
Working in longevity, I came to a rather disappointing conclusion. It is clear that lifestyle has a major impact on longevity., people have great difficulty changing.
Here is my list:
Key lifestyle factors influencing Longevity
- Exercise
- Quality sleep
- Metabolic health
- Social connection
- Cardiovascular prevention
- Avoid smoking
- Cognitive engagement
- Purpose/meaning
- Nutrition quality
- Stress management
Lifestyle probably contributes 50% to longevity while the other 50% is genetics. And there is also an interaction between the two. We cann’t do much about our genetics so we focus on lifestyle.
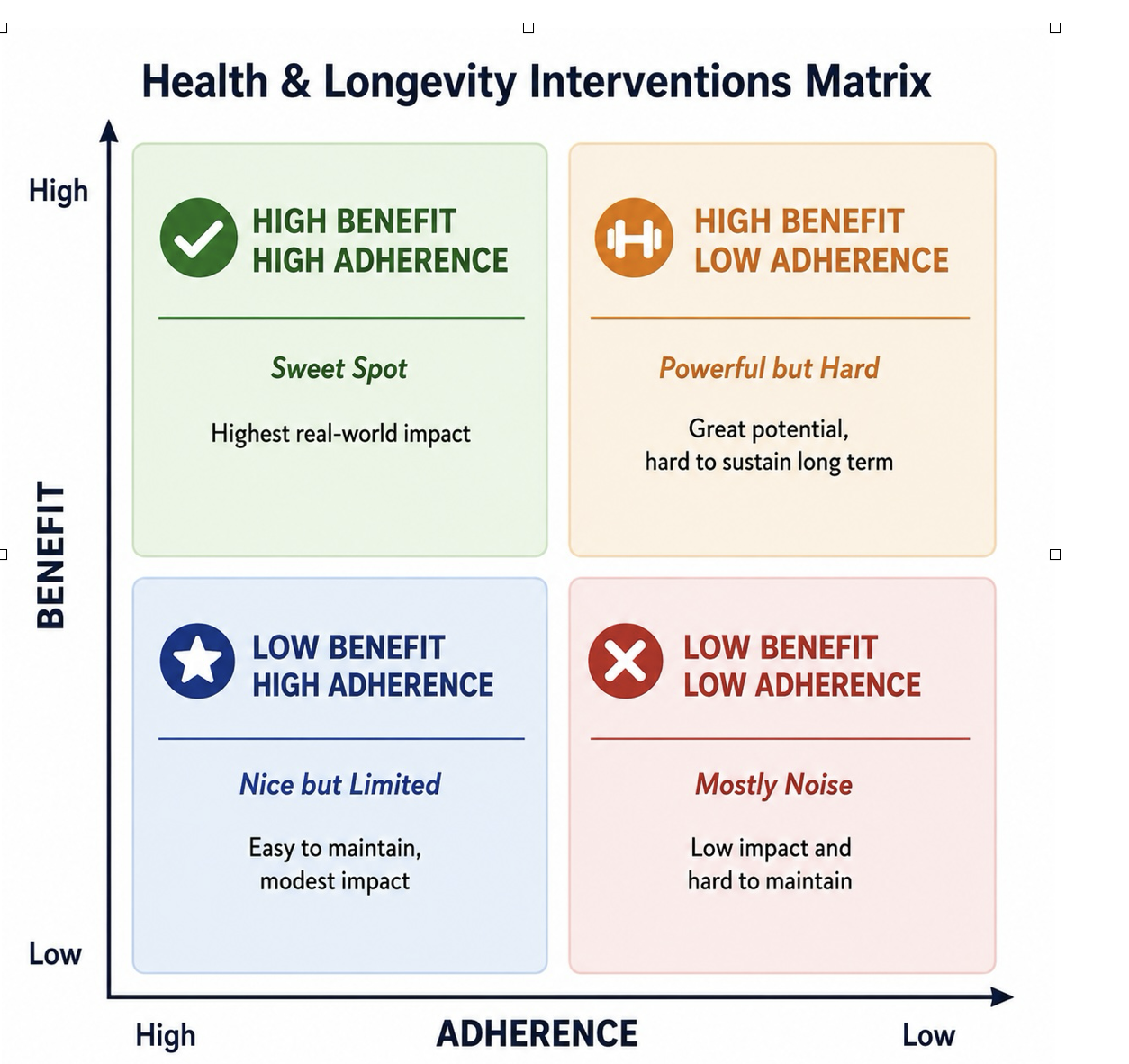
When we first started working on the creation of the Longevity Center at Sheba about five years ago, I made a 2 X 2 matrix in a discussion with Tzipi Strauss, the Director of the institution. I asked her to put different things people could do, like exercise and weight control, into the matrix. The point I would make is that most of the things that give high benefit are in the quadrant of high benefit but low adherence. It was at that point that I began to think that the issue was more about marketing than science. How could we get people to do the things that would keep them healthy? Not that there are no benefits to studying longevity. For instance, I don’t believe in “one size fits all,” which is also where genetics plays a role. It would be best if we knew what factors were the most important per person. This is where precision medicine plays a role.
There are people capable of making lifestyle changes but they are the minority. The bulk of people will need a different kind of help.
This is also important with respect to medical interventions like medication. For instance, taking statins for high cholesterol can be very important for some and not important at all for others. The same is true for blood pressure.
I came to the conclusion that real progress in increasing longevity and in particular health span would come from improvements in pharmaceuticals and not lifestyle changes. Remember, this was all before AI came on to the stage. And this was before GLP-1 drugs took off.
GLP-1 changes everything
GLP-1 (Glucagon-Like Peptide-1) is a natural hormone produced in the intestine after eating that helps regulate appetite, blood sugar, digestion, and feelings of fullness. GLP-1 drugs mimic this hormone, helping people eat less, feel satisfied longer, lose weight, and improve blood sugar control. In addition to treating diabetes and obesity, these medications are increasingly being studied for their broader effects on cardiovascular health, inflammation, addiction, and potentially even longevity.
- Ozempic — semaglutide, primarily for type 2 diabetes
- Wegovy — higher-dose semaglutide for obesity and weight loss
- Mounjaro — tirzepatide for type 2 diabetes
- Zepbound — tirzepatide for obesity and weight loss
- Rybelsus — oral (pill form) semaglutide for type 2 diabetes
A few key points:
- GLP-1 prescriptions increased roughly 10-fold to 40-fold depending on the population studied between 2018–2025.
- Spending on GLP-1 drugs in the U.S. rose from about $13.7 billion in 2018 to over $71 billion in 2023.
- Semaglutide drugs like Ozempic and Wegovy drove the initial explosion, while tirzepatide drugs like Mounjaro and Zepbound are now growing even faster.
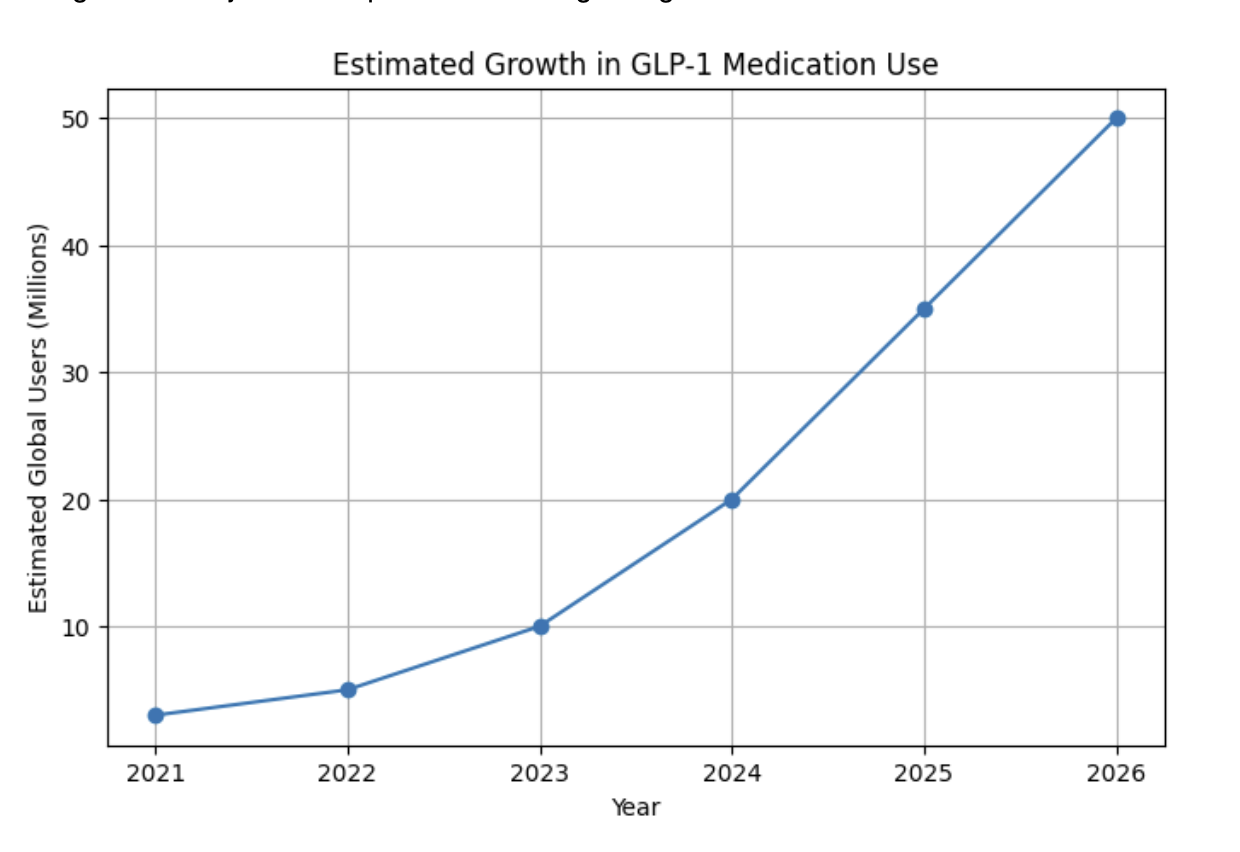
By 2030 we could see as much as 300 million people using these drugs.
And there are innovations coming that could dramatically change this trajectory, including pills instead of injections and dramatically reduced prices. One out of eight Americans is currently using these drugs. I suspect that over 25% of Americans will be using some form of these drugs by 2030.
A Brief History of GLP-1 Drugs
The story of GLP-1 drugs is one of the most remarkable and unexpected developments in modern medicine. What began as research into diabetes has evolved into a global movement that may ultimately reshape obesity treatment, preventive medicine, and even human longevity.
GLP-1 stands for Glucagon-Like Peptide-1, a natural hormone produced in the intestine after eating. Scientists discovered that this hormone plays an important role in regulating blood sugar, slowing digestion, reducing appetite, and increasing feelings of fullness. The problem was that natural GLP-1 breaks down in the body within minutes, making it impractical as a treatment.
The breakthrough came from an unlikely source: the venom of the Gila monster, a venomous lizard found in the southwestern United States and Mexico. In the 1990s, researchers discovered a compound in the lizard’s saliva called exendin-4, which acted similarly to GLP-1 but lasted much longer in the body. This discovery eventually led to the development of the first GLP-1 drug, Byetta (exenatide), approved by the FDA in 2005 for the treatment of type 2 diabetes.
Not just for diabetes
Initially, these drugs were viewed primarily as diabetes medications. Patients taking them often lost weight, but this was considered a secondary effect. Over time, however, it became increasingly clear that their weight loss was not only significant but potentially transformative. Newer generations of GLP-1 drugs were developed that were more effective, longer-lasting, and easier to use. Imagine what the executives thought when they realized what they had discovered.
The next major milestone came with semaglutide, developed by the Danish pharmaceutical company Novo Nordisk. Semaglutide was marketed under different brand names, including Ozempic for diabetes and Wegovy for obesity. Clinical studies showed unprecedented levels of weight loss for a medication, with many patients losing 15% or more of their body weight.
Soon afterward, Eli Lilly and Company introduced tirzepatide, marketed as Mounjaro for diabetes and Zepbound for obesity. Tirzepatide targeted not only GLP-1 receptors but also another metabolic pathway called GIP (Glucose-Dependent Insulinotropic Polypeptide). In many studies, tirzepatide produced even greater weight loss than semaglutide, with some patients approaching the results previously achievable only through bariatric surgery.
As millions of people began using these medications, researchers noticed something important: the effects extended far beyond weight loss. GLP-1 drugs significantly reduced the risk of heart attack and stroke, improved blood sugar control, reduced inflammation, and appeared to positively influence fatty liver disease, kidney disease, and sleep apnea. Researchers also began investigating possible effects on addiction, compulsive behavior, Alzheimer’s disease, and Parkinson’s disease.
This broader impact has led many scientists to believe that GLP-1 drugs may represent something historically unusual: medications that alter not just a disease process, but human behavior itself. Many users describe a reduction in “food noise” the constant mental preoccupation with eating. Others report reduced cravings for alcohol, smoking, and other compulsive behaviors. Some researchers now speculate that the long-term significance of GLP-1 drugs may lie as much in behavioral regulation as in metabolism.
A spectacular adoption curve
The rise of GLP-1 drugs has also created one of the fastest adoption curves in pharmaceutical history. Within only a few years, millions of Americans began using these medications, and demand rapidly spread globally. Analysts now project that tens of millions, and possibly hundreds of millions, of people worldwide may eventually use GLP-1 or related metabolic drugs.
At the same time, important questions remain unanswered. The drugs are expensive, side effects can occur, and many people regain weight after stopping treatment. It is still unclear how long patients should remain on the medications, whether they should eventually be used preventively in healthy individuals, and what the long-term societal consequences will be.
Nevertheless, it is increasingly clear that GLP-1 drugs represent far more than a new category of weight-loss medication. They may mark the beginning of a new era in medicine, one focused not simply on treating disease after it occurs, but on altering the metabolic and behavioral pathways that contribute to aging, chronic illness, and reduced health span.
Not just diabetes and weight loss
Although GLP-1 drugs were originally developed to treat type 2 diabetes, researchers soon discovered that they produced significant weight loss by reducing appetite and increasing feelings of fullness. Since then, it has become increasingly clear that these medications have effects far beyond diabetes and obesity. Researchers are now studying their impact across a wide range of metabolic, cardiovascular, neurological, and behavioral conditions. The top potential benefits currently associated with GLP-1 drugs include:
- Weight loss and obesity reduction
- Improved blood sugar control in type 2 diabetes
- Reduced risk of heart attack and stroke
- Lower blood pressure and improved cardiovascular health
- Reduced inflammation throughout the body
- Improvement in fatty liver disease (NAFLD/NASH)
- Better kidney protection and slower progression of kidney disease
- Improvement in sleep apnea symptoms through weight reduction
- Reduced cravings and compulsive behaviors, including possible effects on alcohol and smoking addiction
- Potential neuroprotective effects being studied in Alzheimer’s disease and Parkinson’s disease.
Like all medications, GLP-1 drugs can produce side effects, although most are gastrointestinal and often improve over time as the body adapts. The most common side effects include nausea, vomiting, diarrhea, constipation, bloating, and reduced appetite. Some people experience fatigue, dizziness, or acid reflux, particularly when starting treatment or increasing dosage. Because these drugs slow stomach emptying, they can occasionally cause more serious digestive problems, including severe nausea in susceptible individuals. Rapid weight loss may also contribute to loss of muscle mass if protein intake and exercise are inadequate. Rare but more serious concerns include pancreatitis, gallbladder disease, and possible thyroid-related risks observed in animal studies. Another important issue is that many people regain weight after stopping the medication, suggesting that long-term treatment may be necessary for sustained benefit. Despite these concerns, most physicians currently view the overall risk-benefit profile of GLP-1 drugs as highly favorable for people with obesity, diabetes, or significant metabolic disease. It is important to maintain muscle mass by exercising and eating protein.
The Economic Impact of GLP-1 Drugs
The rise of GLP-1 drugs may ultimately become one of the largest economic events in the history of healthcare. These medications are already reshaping pharmaceutical markets, insurance systems, food industries, and employer healthcare costs. But their long-term impact could extend much further, potentially altering national healthcare spending, workforce productivity, retirement economics, and even demographic trends.
The immediate economic effect is obvious: GLP-1 drugs are expensive. In the United States, annual treatment costs can exceed $10,000 per person, and tens of millions of people may eventually use them. This creates enormous short-term costs for insurers, governments, and employers. At first glance, widespread adoption appears financially unsustainable.
However, supporters argue that the drugs may dramatically reduce the downstream costs associated with obesity and metabolic disease. Obesity contributes to some of the most expensive chronic conditions in modern society, including type 2 diabetes, cardiovascular disease, stroke, kidney failure, sleep apnea, joint disease, and fatty liver disease. These conditions generate enormous long-term healthcare expenditures, disability costs, and lost productivity.
If GLP-1 drugs significantly reduce obesity and improve metabolic health across large populations, the savings could be substantial. Fewer heart attacks, fewer strokes, less dialysis, fewer diabetes complications, and lower hospitalization rates could offset a meaningful portion of the cost of the drugs themselves. Employers may also benefit from reduced absenteeism, increased productivity, and healthier aging workforces.
But there is another side to the equation. If these drugs truly extend health span and longevity, they may also increase the long-term costs associated with aging populations. People who avoid cardiovascular disease and diabetes may live longer, remain healthier longer, and require less medical care during middle age. But they will also spend more years collecting pensions, Social Security, and retirement benefits.
This creates a fascinating economic paradox. Historically, many healthcare costs were concentrated in the final years of life. If GLP-1 drugs delay disease and extend healthy life, society may save money on chronic illness while simultaneously increasing the number of years people remain alive. In other words, reducing obesity-related disease may lower medical costs but increase retirement and longevity-related costs.
The broader economic implications could be profound. Governments may eventually face difficult questions about retirement age, pension systems, workforce participation, and the economics of aging societies. If millions of people remain healthier into their seventies and eighties, traditional assumptions about retirement may begin to change. Longer health span could allow many people to work longer, remain productive longer, and contribute economically for additional years.
There may also be major second-order effects across industries. Food companies are already reporting changes in consumer behavior among GLP-1 users, including reduced consumption of snacks, alcohol, and highly processed foods. Airlines may benefit from lower passenger weight. Healthcare systems may shift resources away from late-stage metabolic disease. Pharmaceutical companies are investing billions into next-generation metabolic drugs that may become one of the largest drug categories in history.
In many ways, GLP-1 drugs sit at the intersection of medicine, economics, and demography. They may reduce some of the largest chronic disease burdens of modern civilization while simultaneously accelerating one of the central challenges of the twenty-first century: how societies adapt to populations that live longer and stay healthier for more years.
Different reactions by different governments
Governments around the world are taking very different approaches to GLP-1 drugs because they are balancing competing concerns involving healthcare costs, obesity, diabetes, workforce productivity, and aging populations. In the United States, adoption has been rapid and largely market-driven. High obesity rates, aggressive pharmaceutical marketing, and strong consumer demand have made America the largest GLP-1 market in the world. At the same time, insurers and government programs are struggling with the enormous short-term costs of these medications, creating ongoing debates about reimbursement and access.
European countries have generally taken a more cautious and cost-controlled approach. Because most European healthcare systems are government-funded, decisions are heavily influenced by cost-effectiveness analysis. Many countries restrict reimbursement to patients with severe obesity or diabetes and carefully evaluate whether the long-term health savings justify the immediate expense. Nevertheless, rising obesity rates and aging populations are increasing European interest in these drugs as potential tools for reducing future healthcare burdens.
China may ultimately become one of the most important GLP-1 markets in the world. The country faces rapidly rising obesity and diabetes rates, along with the economic challenges of an aging population. Chinese policymakers increasingly view metabolic disease as both a public-health and economic threat. At the same time, China is investing aggressively in domestic biotechnology companies that are developing lower-cost GLP-1 alternatives and next-generation metabolic therapies. In this sense, China appears to view GLP-1 drugs not only as healthcare products, but also as strategic biotechnology infrastructure.
The Gulf states, including Saudi Arabia and the UAE, are also showing strong interest because they have some of the highest obesity and diabetes rates in the world. In contrast, Japan has moved more cautiously due to lower obesity rates and a traditionally conservative medical culture. Across much of the developing world, affordability remains the largest barrier, although lower-cost manufacturing and future generic versions could eventually expand access dramatically.
What makes GLP-1 drugs so economically and politically important is that governments increasingly understand that metabolic disease is not simply a healthcare issue. It affects workforce productivity, military readiness, healthcare spending, disability rates, and the economics of aging societies. If these drugs continue to prove effective and safe, they may eventually be viewed less as obesity medications and more as part of the core infrastructure of preventive medicine.
One of the most important questions surrounding GLP-1 drugs is whether they will ultimately extend human lifespan and health span. The honest answer is that nobody yet knows with certainty. These drugs are still relatively new, and we do not yet have decades of long-term data showing their direct effect on longevity. However, based on what we already know about obesity, diabetes, cardiovascular disease, and metabolic health, there are strong reasons to believe that for many people the impact could be substantial.
GLP-1 drugs probably do not slow aging directly in the way science fiction often imagines. Instead, they appear to reduce many of the major biological processes that accelerate aging and shorten life. Obesity and metabolic disease contribute to inflammation, vascular damage, high blood pressure, fatty liver disease, kidney disease, sleep apnea, and cardiovascular disease — all of which are strongly associated with reduced lifespan and diminished quality of life. By improving metabolic health and reducing these risks, GLP-1 drugs may indirectly slow some of the most important drivers of aging-related decline.
Importantly, the potential longevity benefit is unlikely to be the same for everyone. For people with severe obesity, diabetes, or significant cardiovascular risk, the impact could be dramatic, potentially adding years of healthy life. For people who are already lean, physically active, and metabolically healthy, the benefit may be much smaller. This may ultimately become one of the most important principles of longevity medicine: the value of an intervention depends heavily on the biological vulnerabilities of the individual.
In many ways, the greatest impact of GLP-1 drugs may not simply be weight loss itself, but the possibility of extending health span; the number of years people remain healthy, active, independent, and cognitively engaged. If these drugs significantly reduce heart attacks, strokes, kidney disease, frailty, and disability, they could reshape not only medicine, but also the economics and demographics of aging societies.
The population pyramid inverts even more
I have been studying the inversion of the population pyramid for the last few years. I became very interested in this phenomenon when I moved to Italy more than a year ago. All the world’s developed nations with the exception of Israel have negative birthrates. This results in increases in the median average age but, more importantly, in the ratio of people working to people retired, putting an increasing burden on the productive people. The good news about GLP-1 is that it should increase health span, the years we are well, but this will also result in increased life span. Who will pay for these years? That is the subject of future blog posts.
One of the great paradoxes of longevity medicine is that success creates new societal challenges. If GLP-1 drugs significantly extend health span — and ultimately lifespan — they may also intensify one of the defining demographic problems of the twenty-first century: the inversion of the population pyramid.
For most of human history, societies had large numbers of young people supporting relatively small elderly populations. That balance is now reversing across much of the developed world. Birth rates are falling while life expectancy continues to rise. As a result, fewer working-age people are supporting larger retired populations through pensions, healthcare systems, and social services.
If GLP-1 drugs and other longevity interventions substantially reduce obesity, diabetes, cardiovascular disease, and age-related disability, millions of people may live longer and remain healthier for more years. On one hand, this could dramatically reduce the cost of chronic illness and improve quality of life. On the other hand, it could increase the number of years people spend collecting retirement benefits, pensions, and government healthcare support.
Check out this wonderful YouTube interview by Ezra Klein for additional sight.
This creates a fascinating economic tension. The success of preventive medicine may simultaneously reduce disease while increasing the long-term financial burden associated with aging populations. In effect, societies may trade the costs of chronic illness for the costs of longevity.
The ultimate solution may not be shorter lives, but rather rethinking the structure of work, retirement, and productivity itself. If people remain healthier into their seventies and eighties, traditional assumptions about retirement age may no longer make economic or social sense. Extending health span may eventually require societies to redefine not only how long people live, but also how long they remain economically and socially engaged.
My own experience with GLP-1
I have been taking Mounjaro, a GLP-1 medication, for about a year and a half. I was not overweight. My BMI was about 25, but I had a belly. I had metabolic syndrome, which can result in a number of diseases. Also, it is not attractive, at least in my opinion (and I am vain). My wife always struggled to lose weight. Her weight affected her view of herself. She tried many things to lose weight but was not successful. We both used intermittent fasting and low carb diets. I think they helped us not gain additional weight. Then she started taking Mounjaro about two years ago and the pounds just melted away. She reached her ideal weight after about nine months. She did not have any side effects. I was impressed and decided to try it myself. I started out with 2.5 mg for about four weeks and then went to 5 mg weekly after that. She then continued on 5 mg but moved to every two weeks.
I started on 2.5 mg and never had to move to a higher dose. I now take that every 10–14 days. I monitor my weight to decide when to take a dose.
I lost 20 pounds over about six months and have maintained this loss.
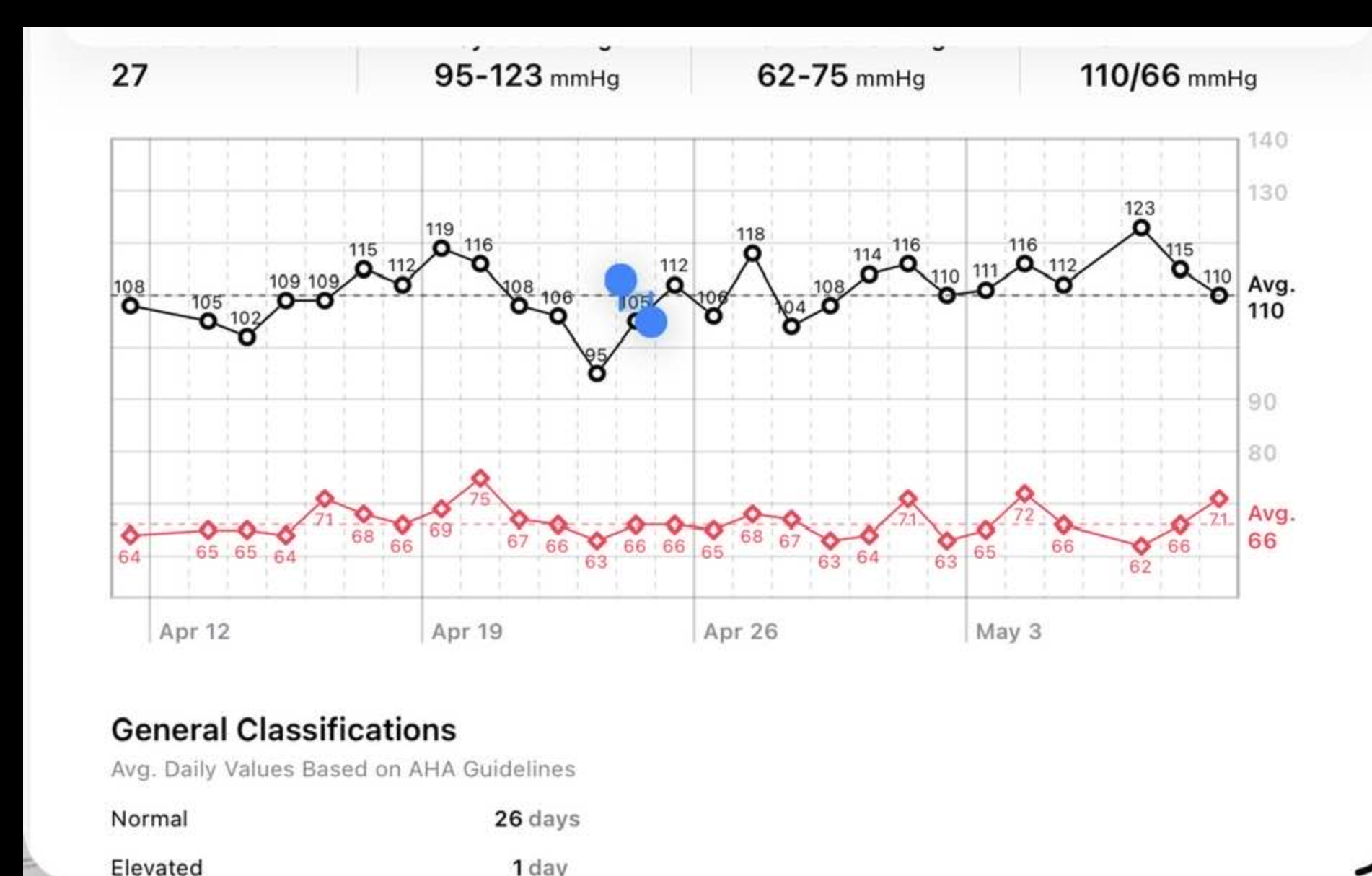
But what was remarkable was the impact on other things. For instance, I had been taking blood pressure medicine for many years. My blood pressure was something like 135/80. Not super high for someone my age. After taking GLP-1 and losing the weight, I no longer have high blood pressure and I take no medication.
Most of my labs have shown improvements, especially inflammation markers. I take statins for high cholesterol. I stopped taking them and was still in the normal range. I went back to taking them because I want to keep my LDL around 60 mg/dL. My HDL is 70 mg/dL. I continue because there is some evidence this will reduce the amount of plaque I already have.
My only side effects are some constipation and not sleeping as well on the night after I’ve taken a shot.
Can we afford to live longer?
The arrival of GLP-1 drugs represents more than a pharmaceutical breakthrough; it marks a fundamental shift into the “Sweet Spot” of longevity science. By creating a high-adherence path to metabolic health, we are beginning to solve the biological puzzles that have historically shortened our health spans. While my own experience with these markers has been transformative, the widespread success of such interventions will eventually force us to confront a significant demographic paradox. As we successfully invert the population pyramid and extend the years we remain active and independent, we must rethink how society will fund and find purpose in this new era of longevity. Unless GLP-1 decreases the incidence of cognitive disorders, we could easily see the number of people suffering from this affliction double.
GLP-1 is a breakthrough for our bodies, but we likely need one for our brains.

Phenomenal and incisive narrative.
LikeLike